Rhinoplasty
Rhinoplasty, or nasal reshaping, is a procedure to change the appearance of the nose. The usual candidates for this procedure are patients who 1) have never felt their noses fit their faces or 2) acquired a change to their nose due to trauma or aging. There are a number of ways to alter the bridge, tip, and nostrils. The nose is the centerpiece of the face, and even subtle changes have a dramatic impact. Every face looks best with a natural-looking nose that is well-proportioned. After rhinoplasty, your nose should look like one you could have been born with.
Most plastic surgeons consider rhinoplasty to be a difficult operation due to the complicated anatomy and potential effects on breathing. Any change to the external appearance of the nose (e.g. making the nose smaller, narrower, straighter, etc.) may make your airway smaller. We take this into account and make the necessary internal improvements to your airway. The last thing we want is an attractive nose that doesn’t work well! Fear not, as facial plastic surgeons are not only trained in cosmetic rhinoplasty but also nasal airway procedures.
Types of Rhinoplasty
Open Rhinoplasty
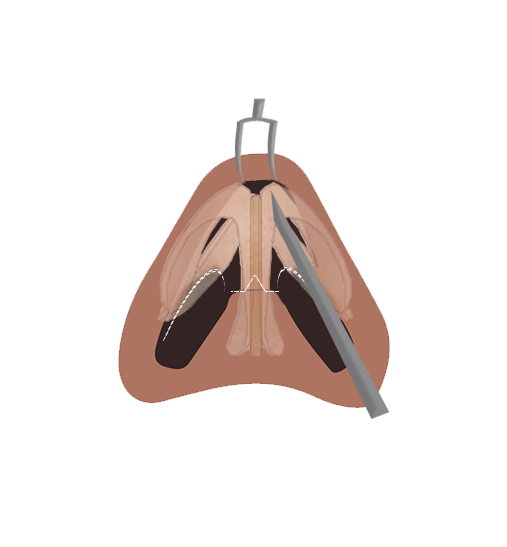
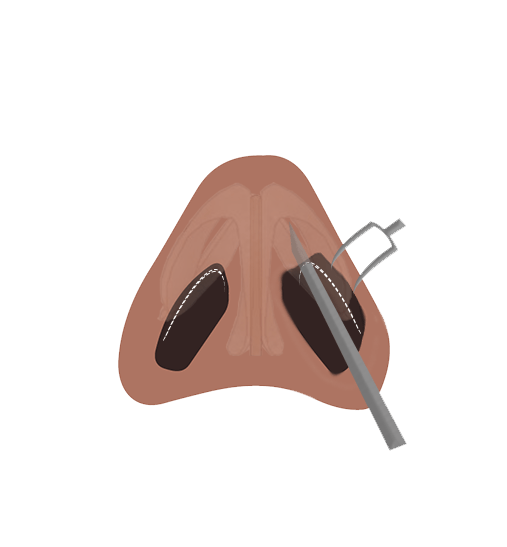
Open rhinoplasty, aka external rhinoplasty, involves one small external incision located between the nostrils on the underside of the nose. The remaining incisions are hidden inside the nostrils. The tip of the nose is then opened to gain full view and access to the underlying structure. This technique allows the most accurate and precise modifications.
Ideal For: Major tip and bridge modifications and revision rhinoplasty.
Closed Rhinoplasty
Endonasal rhinoplasty, aka "endonasal" or “incisionless” rhinoplasty, involves only incisions hidden inside the nose. This allows a shorter procedure and speedier recovery, but less visualization for complex maneuvers as compared to the open rhinoplasty.
Ideal For: Minor modifications to the bridge and tip of the nose.
Tip Rhinoplasty
Tip rhinoplasty only involves the nasal tip. The nasal tip position and definition can be improved by sculpting the underlying nasal cartilage and soft tissue. The tip can be positioned closer or farther from the face or may be turned up or down. The procedure may or may not involve an external incision.
Ideal For: Those who are only concerned with the shape of the tip of their nose and do not need modifications to the bridge.
Revision Rhinoplasty
Revision rhinoplasty, aka secondary rhinoplasty, is arguably the most difficult facial cosmetic operation due to scarring and alterations in structure from the previous rhinoplasty. Usually, it is performed a year or more after the previous procedure to allow proper healing. The extent of revision varies – in some, it may be a small modification to the nostril or tip, while in others, major bridge or tip work may be necessary. The degree of surgery dictates the type and extent of incisions required. With major revisions, we often need cartilage grafts from the septum, ears, or rib to accomplish our goals.
Ideal For: Correcting previous rhinoplasty results.
Non-Surgical (Liquid) Rhinoplasty
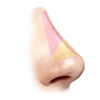
Non-surgical rhinoplasty, aka liquid rhinoplasty, may be an option for patients who are unhappy with their nose but are not yet ready for invasive rhinoplsty. Filling the area around the bump creates the illusion of a perfectly straight nose. This cosmetic treatment is not meant to decrease nose size; instead, the nose appears smaller when it looks straighter.
Dr. Patel uses the filler Radiesse for most nonsurgical rhinoplasty treatments. This filler creates structure and a firm hold--ideal for placement in the nose. Patients often find this product lasts longer than other brands of fillers. The injection process itself takes less than 5 minutes and a full correction may be accomplished in one to two treatments with little if any downtime.
Injection rhinoplasty is not a substitution for rhinoplasty. These fillers can improve the shape and contour of your nose but effects are temporary, usually lasting over a year, and are only suitable for some instances.
Ideal For: Someone with a noticeable bump or crooked bridge that is not ready for an invasive procedure.
Planning Your Procedure
Pre-Operation
Surgery
Post-Operation
Nasal Anatomy 101
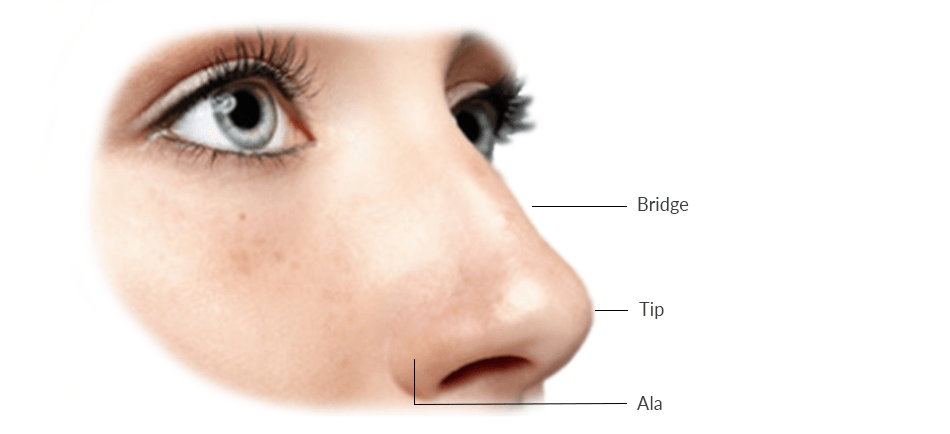
The bridge is formed by hard bone on the upper half and softer cartilage on the lower half. The lower half of the bridge also houses the nasal valve area, which is critical for nasal breathing. The nasal septum runs right down the middle of the entire bridge and often dictates straightness of your nose. On the profile, we prefer the bridge to be relatively straight from top to bottom. In females, a light inward slope is often desirable. In men, a slight outward slope may look attractive. From the front, the bridge should be straight and project forward to a gently rounded apex. The width of the bridge should resemble an hourglass from top to bottom.
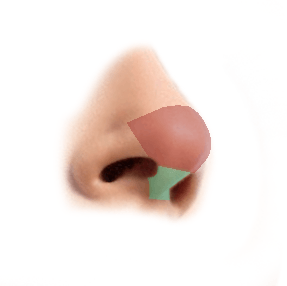
The tip is formed by two arched cartilages with one common leg, resembling a three-legged stool. The upper legs extend above the nostrils, while the lower, common leg spans the columella (the fleshy part between the nostrils). There is a wide variety in their width, height, curvature, and overall shape. With a refined nasal tip, these cartilages have a strong bend in the arched region and the tripod legs are straight and strong.
The ala is the fleshy part that houses the nostrils. There is no cartilage in this region. The floor of the nostril opening between the ala and columella is called the nasal sill. Nostril show is influenced by the position of the nasal tip, position of the columella (fleshy part between the nostrils), and arch of the nostrils. Ideally, the nasal tip should project straight out from the face, the columella should hang down a little lower than the nostrils, and the nostril margins should have a gentle arch.
Common Nose Shape Concerns
Postoperative Care
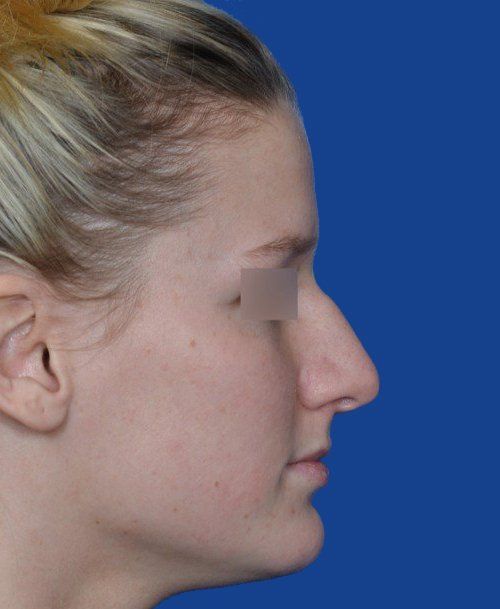
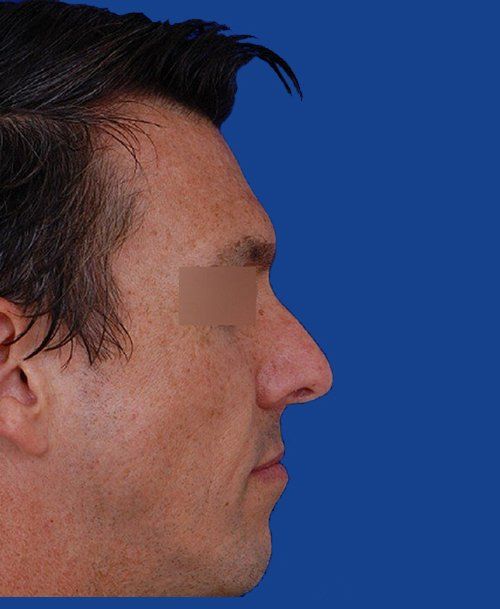
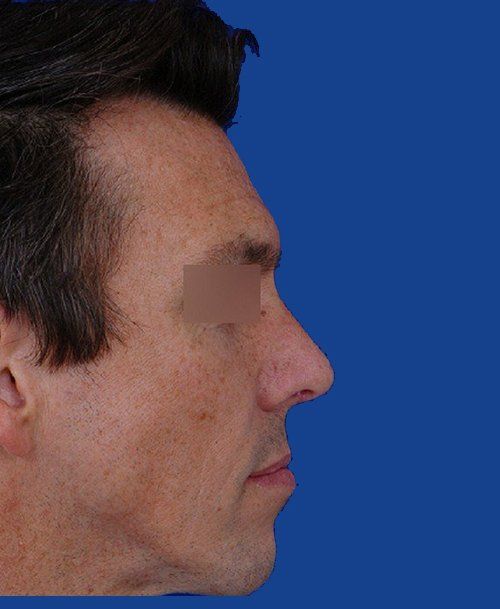
Patient Transformations

Related Blog Posts